


Giving Up the Belief in Flu Shots
Truth Tellers Sound like Raving Lunatics


Influenza vaccines have been in use for more than 60 years. One of the earliest clinical trials of influenza vaccine efficacy was conducted in United States Army personnel in 1943. Approximately 11,000 unvaccinated young men received a flu shot that had one strain of both influenza type A and type B. The study’s endpoint - the development of a febrile illness - showed that 7.1% of unvaccianted recruits developed a fever vs. only 2.2% of the vaccinated became sick. This early study assumed the fever was caused by influenza viruses and if they didn’t get sick, the success could be attributed to a flu shot.
The problem with this ‘end point’ is that many different viruses and bacteria can cause febrile illness, often referred to as influenza-like illness (ILI). For example, there are at least 52 immunologically distinct adenoviruses (different types) that can cause human illness. According to the Centers for Disease (CDC), there are about 30 strains of coronaviruses. Seven strains are known to infect humans and most commonly cause upper respiratory tract illness (a cold) or flu-like illness.
After a few more military trials, the assumption for the success of influenza vaccines lead to widespread influenza vaccine use in civilian populations in 1960. The U.S. Public Health Service (USPHS) recommended annual vaccination of adults aged ≥65 yr, pregnant women (no safety studies then either!!), and those with chronic illness.
The impact was disappointing. Four years later (1964), a review of the program by USPHS leaders concluded:
“An appraisal of experience for the past three and a half years indicates little progress in control of influenza. The basic assumptions of the control program must be reassessed. There is little evidence that recent vaccines have significantly prevented clinical illness, as well as equally little evidence to evaluate effects on mortality. How long such a program should be continued without better scientific evidence is problematic. Sounder bases are needed for an influenza control program.”
Fast forward: 2005
On September 21, 2005, The New York Times published a ground-breaking story reporting on a study with strong evidence that flu shots are ineffective and possibly even harmful in the most highly targeted group, the elderly. Published in The Lancet Online (September, 2005), the study provided no new data but reviewed 64 existing studies that evaluated the effectiveness of the flu vaccine over 96 flu seasons. The authors concluded that the effectiveness of flu shot—particularly in the elderly—was “wildly overstated.”
“The runaway 100 percent effectiveness that’s touted by proponents [of the flu shot] was nowhere to be seen,” said Dr. Thomas Jefferson, a Rome-based researcher with the Cochrane Vaccine Fields project, an international consortium of scientists who perform systematic reviews of research data. “What you see is that marketing rules the response to influenza vaccines, and scientific evidence comes fourth or fifth. Vaccines may have a role, but they appear to have a modest effect. The best strategy to prevent the illness is to wash your hands.”
Not much has changed in the last 15+ years in terms of identifying the efficacy of flu shots. Unlike other vaccines, influenza vaccine efficacy is a moving target due to all the annual mutations, including changes that occur on the surface proteins even while they are replicating in their egg incubators.
A paper published in 2020 by Leigh Krietsch Boerner as much as admits that the chance of the viruses grown in eggs, extracted and the put into the annual flu shot are not going to ‘match’ the viruses in circulation.
Recent evidence has emerged that the efficacy of flu shots can also be affected by how the pharmaceutical industry makes its vaccines. Most flu shots are currently produced from viruses grown in chicken eggs containing an embryo. Scientists have observed that mutations can occur in influenza viruses grown inside such avian cells, potentially leading to vaccines that are less effective because they are aimed at a slightly different version of the virus than the one we’re exposed to.
The truth is, flu shots are mostly ineffective. It has long been known that when circulating viruses do not match the vaccine strains, vaccination provides little to no protection. In the best years, flu shots show can show an efficacy rate of up to 60%; some years, effectiveness plunges to as low as 10%. This discrepancy is based on how well manufacturer’s have ‘guessed’ which strain to include in the current year’s slurry.
Looking at Current ‘Efficacy’ Data
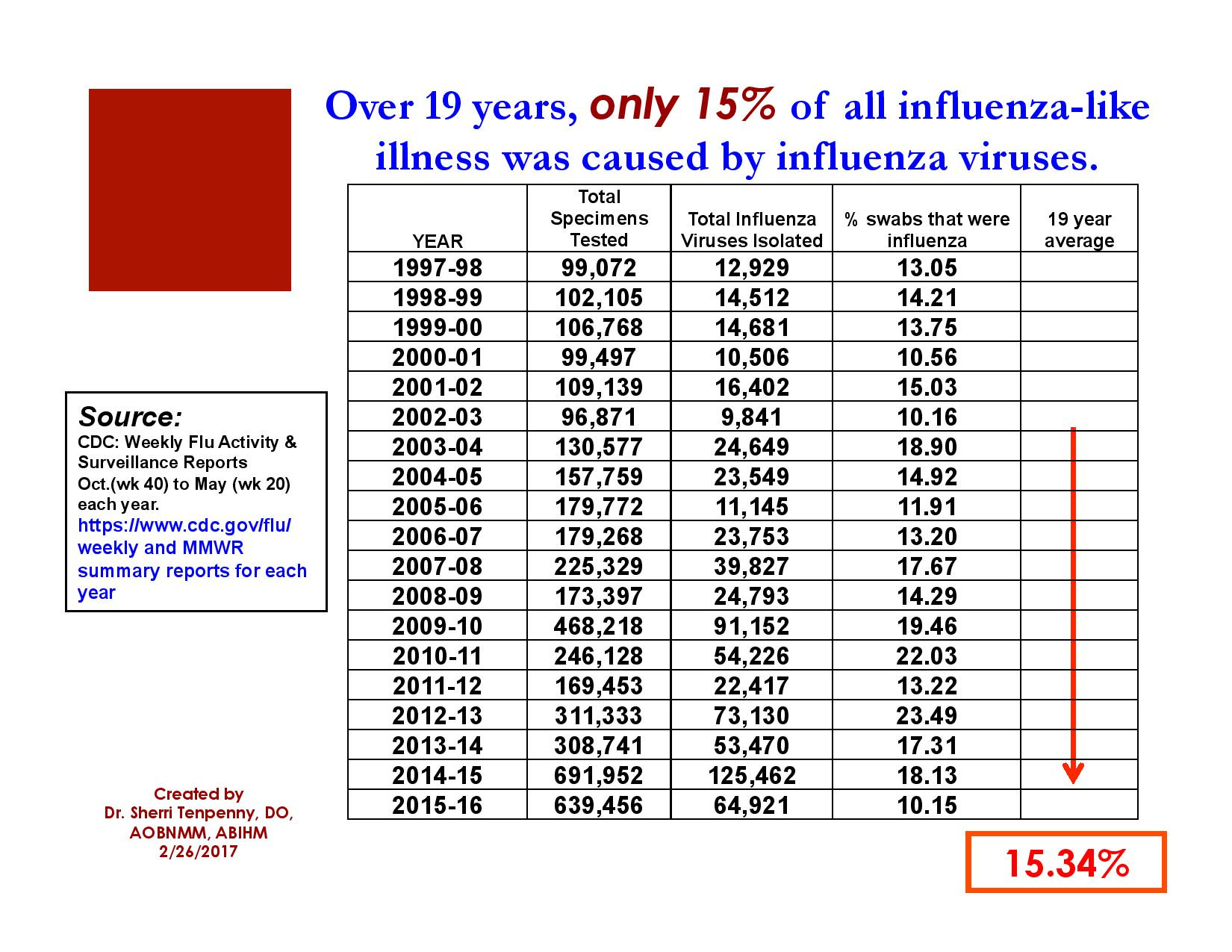
A few years back, I did an evaluation of the data gathered and collated each week by the CDC during influenza season. Weekly flu activity and surveillance reports are generated from October (wk 40) to May (wk 20) of the following year. Hundreds of thousands of swabs are tested each season. The first step determines if the sample, taken from a person with flu-like symptoms, is positive or negative for influenza viruses. If the sample IS positive, the viruses are then sub-typed; this is how the CDC determines if the viral strains in the flu shots are ‘a match’ to the viruses causing community illness.
Remember: If they don’t match, the flu shot you took was all risk and no benefit; it was essentially worthless in preventing you from getting sick.
The same 2020 paper by Boerner (mentioned above) also states this:
Flu viruses that develop mutations in their surface proteins during vaccine manufacture may no longer match the ones circulating in the wild, and therefore the vaccines can’t protect people who receive shots as well.
Hmmm.
I analyzed the data from the 1997/98 flu season up through the 2015/16 flu seasons. Here’s the table I created, showing that in any given flu season, only 15.34% of illness was caused by influenza viruses. That means the flu shot was worthless almost 85% of the time in preventing the flu; it’s even MORE worthless if the viruses in the positive samples don’t match the serotypes that are in that year’s flu shot!
To be more current, I looked at the most recent available data for the current 2022 influenza season.
Cumulative data through October 2, 2022 (wk 40)
575,479 specimens tested
49,726 specimens were *positive* for influenza A or B (8.6%)
In Week 45 alone (Oct. 30 to Nov. 5, 2022) ==> The Beginning of ‘Sugar Season’!
103,830 specimens tested
15,308 specimens were *positive* for influenza A or B (14.7%)
So, not much has changed since 2016, and I’m sure the data in the intervening years is similar. You can see the numbers for yourself by going here. (scroll down).
For Flu Shot Devotees
I know that most who are reading this column avoid flu shots like the plague. But I’m sure you have many friends and family members who rush out to get their flu shot each season like it was as good for them - and as harmless - as a B-12 shot.
If they listen to you at all, learning that flu shots, similar to the Covid shots offer risk but no benefit is disturbing, The reaction to this information is predictable. Many people will deny it. Then many more will become angry and call it ‘misinformation.’ Denial is most pervasive among doctors and public health officials who encourage everyone to “get your flu shot NOW!” despite convincing evidence that they don’t protect you from getting the flu.
Denials from friends and family may sound something like this:
“Well, the flu shot always protects me.”
“Shouldn’t some people get the flu shot?”
“My doctor would never recommend something that wasn’t beneficial or could be harmful. I really LIKE my doctor!”
Reversing the ingrained beliefs about the effectiveness of flu shots is difficult, even in light of solid evidence. Many will never give up their long-held belief that a flu shot protects them from the flu.
I’ll close today with two of my favorite quotes:
The first, by Dresden James, a pen name of the writer Donald James Wheal, said: ‘It wasn’t the world being round that agitated people, but that the world wasn’t flat.’
James is also noted for saying one of my other long time favorite quotes:
“A truth’s initial commotion is directly proportional to how deeply the lie was believed. When a well-packaged web of lies has been sold gradually to the masses over generations, the truth will seem utterly preposterous and its speaker a raving lunatic.”
Welcome to the Club of Raving Lunatics.
The Eye on the Evidence substack is posted each Saturday. I write a second substack, On Walking with God, which is released each Sunday. For more information, here are additional links to my 3 podcasts, my supplement store and my apparel store.
Risk v Benefit
Risk varies with your DNA and the chemicals in the "vaccine" (poison). As one old doctor said, "I have never seen an unvaccinated person get cancer" and others have noted that there were no cases of autism until the vaccines started using aluminium.
no benefit for healthy immune systems
So, eat well, sleep well, exercise regularly, breathe fresh air and drink clean water, have a loving family and you will live a long life without a vaccine.
Here’s another reason not to: From Geert: “I continue to emphasize that in highly vaccinated countries Bird Flu may start to spread asymptomatically via vaccinees and that C-19 unvaccinated who vaccinate against seasonal/common Flu are at high risk of contracting Ab-dependent enhancement of avian Flu disease!”